Ovarian epithelial cancer is the most common type of ovarian cancer. It begins in the tissue that covers the ovaries. This information is not about ovarian germ cell tumors or other types of ovarian cancer.

Ovarian Cancer Experts
Ovarian cancer – words no woman wants to hear. With no known cause, no accurate screening test, and symptoms that are often vague and misdiagnosed, diagnosis of this cancer tends to happen at a more advanced stage, making it one of the more challenging gynecologic cancers to treat. Having an experienced team led by a gynecologic oncology surgeon and a sub-specialized medical oncologist is important to ensure the most advanced treatment options available. At Rocky Mountain Cancer Centers (RMCC) our experts specialize in evidence-based, cutting-edge, and personalized treatment plans to create the best possible outcomes.
Risk Factors & Prevention
Ovarian cancer is one of the more challenging cancers to treat as it isn’t as easily detected as other cancers. Because of this, it’s a good idea to know what factors can put you at an increased risk of developing the disease. Keep in mind that having risk factors for ovarian cancer doesn’t mean you will develop it. Still, being aware will better equip you to make lifestyle choices that can help lower your chance of getting it.
Risk Factors for Ovarian Cancer
There are several factors that can increase your risk of developing ovarian cancer. While many of these, like age and genetics, are out of your control, others that involve personal lifestyle choices can be adjusted to lower risk.
Common risk factors for ovarian cancer include:
- Age. Ovarian cancer is very rare in women under the age of 40. Most ovarian cancers develop after menopause. Half of all ovarian cancers are found in women aged 63 or older.
- Personal history of cancer or endometriosis. Women who have had breast cancer, uterine cancer, or colorectal cancer have a higher risk of ovarian cancer. Having endometriosis increases the risk of clear cell and endometrioid ovarian cancers 2-3 fold.
- Family history. About 5-10% of ovarian cancers are hereditary through a mutation in the BRCA gene. Women who have a first-degree relative (such as a grandmother, mother, daughter, or sister) with ovarian cancer or breast cancer may be at an increased risk. Finding out if there is a BRCA gene mutation in your family is a good place to start. Our genetic counselors can assist you with this. The risk of ovarian cancer is also increased in women with certain inherited syndromes, including familial site-specific ovarian cancer syndrome, familial breast/ovarian cancer syndrome, and hereditary nonpolyposis colorectal cancer (HNPCC; Lynch syndrome).
- Weight and height. Being overweight or having obesity is linked to an increased risk of ovarian cancer. Obesity is also linked to an increased risk of death from ovarian cancer. Being tall may also be linked to a slight increase in the risk of ovarian cancer.
- Reproductive history and infertility. Women who had full-term pregnancies, before the age of 26, are at a lower risk than women who had their first full-term pregnancy after age 35. Women who have never carried a pregnancy to term are also at a higher risk. Each full-term pregnancy lowers your risk. Breastfeeding may reduce the risk as well. Women who started menstruating at an early age (before 12) and/or experienced menopause after age 50 are also at an increased risk.
- Birth control. Using oral contraceptives (birth control pills) for a minimum of 3 to 6 months can lower the risk for ovarian cancer. The risk continues to drop the longer the pills are used. With that said, the use of oral contraceptives can increase your risk for some other health issues, including cervical and breast cancers.
- Hormone replacement therapy. There is a slightly increased risk of ovarian cancer in women who are taking hormone replacement therapy (HRT) after menopause. There is also an increased risk of ovarian cancer in women who have recently used HRT, even if they used it for less than 5 years. The risk of ovarian cancer is the same for HRT with estrogen only or with combined estrogen and progestin. When HRT is stopped, the risk of ovarian cancer decreases over time. The risk of ovarian cancer is not affected by the age of the woman when taking HRT.
Reducing Your Risks of Developing Ovarian Cancer
While there is no guarantee that you won’t get ovarian cancer by taking steps to reduce your risk, there are things you can do to lower your risk including:
- Making better lifestyle choices in regards to diet and exercise.
- Avoiding things that are linked to ovarian cancer, such as talcum powder and smoking.
- Breastfeeding, if you are still in the childbearing stage of life.
- Using birth control pills.
- Having gynecological surgery such as tubal ligation or hysterectomy. This is not a common recommendation unless you have the BRCA gene mutation. Because preventative surgeries like this come with potential risks and side effects, we urge you to talk with your oncologist and/or a genetic counselor if you are considering this.
Diagnosis
If you have a symptom that suggests ovarian cancer, your doctor must find out whether it is due to cancer or to some other cause. Your doctor may ask about your personal and family medical history.
You May Have One Or More Of The Following Tests. Your Doctor Can Explain More About Each Test:
- Physical exam: Your doctor checks general signs of health. Your doctor may press on your abdomen to check for tumors or an abnormal buildup of fluid (ascites). A sample of fluid can be taken to look for ovarian cancer cells.
- Pelvic exam: Your doctor feels the ovaries and nearby organs for lumps or other changes in their shape or size. A Pap test is part of a normal pelvic exam, but it is not used to collect ovarian cells. The Pap test detects cervical cancer. The Pap test is not used to diagnose ovarian cancer.
- Blood tests: Your doctor may order blood tests. The lab may check the level of several substances, including CA-125. CA-125 is a substance found on the surface of ovarian cancer cells and on some normal tissues. A high CA-125 level could be a sign of cancer or other conditions. The CA-125 test is not used alone to diagnose ovarian cancer. This test is approved by the Food and Drug Administration for monitoring a woman’s response to ovarian cancer treatment and for detecting its return after treatment.
- Ultrasound: The ultrasound device uses sound waves that people cannot hear. The device aims sound waves at organs inside the pelvis. The waves bounce off the organs. A computer creates a picture from the echoes. The picture may show an ovarian tumor. For a better view of the ovaries, the device may be inserted into the vagina (transvaginal ultrasound).
- Biopsy: A biopsy is the removal of tissue or fluid to look for cancer cells. Based on the results of the blood tests and ultrasound, your doctor may suggest surgery (a laparotomy) to remove tissue and fluid from the pelvis and abdomen. Surgery is usually needed to diagnose ovarian cancer. To learn more about surgery, see the “Treatment” section.
Although most women have a laparotomy for diagnosis, some women have a procedure known as laparoscopy. The doctor inserts a thin, lighted tube (a laparoscope) through a small incision in the abdomen. Laparoscopy may be used to remove a small, benign cyst or an early ovarian cancer. It may also be used to learn whether cancer has spread.
A pathologist uses a microscope to look for cancer cells in the tissue or fluid. If ovarian cancer cells are found, the pathologist describes the grade of the cells. Grades 1, 2, and 3 describe how abnormal the cancer cells look. Grade 1 cancer cells are not as likely as to grow and spread as Grade 3 cells.
Staging
To plan the best treatment, your doctor needs to know the grade of the tumor and the extent (stage) of the disease. The stage is based on whether the tumor has invaded nearby tissues, whether the cancer has spread, and if so, to what parts of the body.
Usually, surgery is needed before staging can be complete. The surgeon takes many samples of tissue from the pelvis and abdomen to look for cancer.
Your Doctor May Order Tests To Find Out Whether The Cancer Has Spread:
- CT scan: Doctors often use CT scans to make pictures of organs and tissues in the pelvis or abdomen. An x-ray machine linked to a computer takes several pictures. You may receive contrast material by mouth and by injection into your arm or hand. The contrast material helps the organs or tissues show up more clearly. Abdominal fluid or a tumor may show up on the CT scan.
- Chest x-ray: X-rays of the chest can show tumors or fluid.
- Barium enema x-ray: Your doctor may order a series of x-rays of the lower intestine. You are given an enema with a barium solution. The barium outlines the intestine on the x-rays. Areas blocked by cancer may show up on the x-rays.
- Colonoscopy: Your doctor inserts a long, lighted tube into the rectum and colon. This exam can help tell if cancer has spread to the colon or rectum.
These Are The Stages Of Ovarian Cancer:
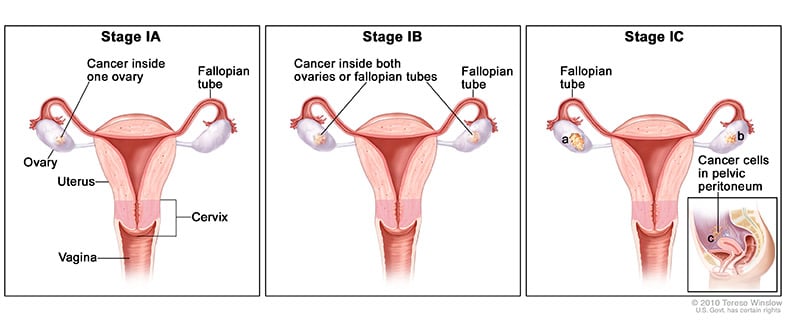
- Stage I: Cancer cells are found in one or both ovaries. Cancer cells may be found on the surface of the ovaries or in fluid collected from the abdomen.
-
Stage IA: The cancer is only inside 1 ovary or fallopian tube. No cancer is found on the ovarian or fallopian tube surface or in the abdomen.
-
Stage IB: The cancer is in both ovaries or fallopian tubes. No cancer is found on the surface of the ovary or fallopian tube or in the peritoneal fluid or washings.
-
Stage IC: The cancer is in 1 or both ovaries or fallopian tubes, with any of the following:
-
Stage IC1: The tumor ruptures while it is being removed surgically, called intraoperative surgical spill.
-
Stage IC2: The tumor wall is ruptured before surgery, or there is cancer on the surface of the ovary or fallopian tube.
-
Stage IC3: Cancer cells are found in fluid buildup in the abdominal cavity, called ascites, or in the samples of fluid from the peritoneal cavity taken during surgery.
-
-
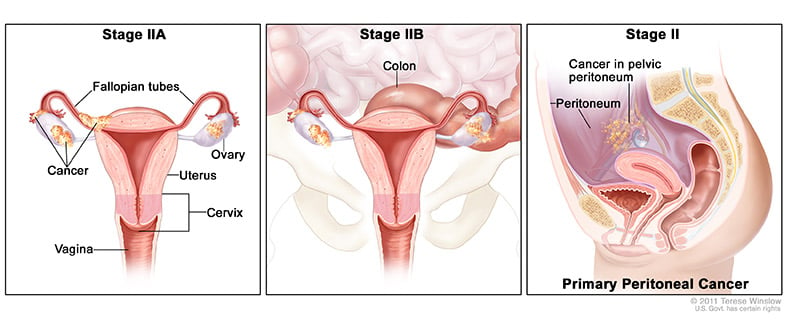
- Stage II: Cancer cells have spread from one or both ovaries to other tissues in the pelvis. Cancer cells are found on the fallopian tubes, the uterus, or other tissues in the pelvis. Cancer cells may be found in fluid collected from the abdomen.
-
Stage IIA: The cancer has spread to the uterus and/or fallopian tubes and/or the ovaries.
-
Stage IIB: The cancer has spread to other tissues within the pelvis.
-
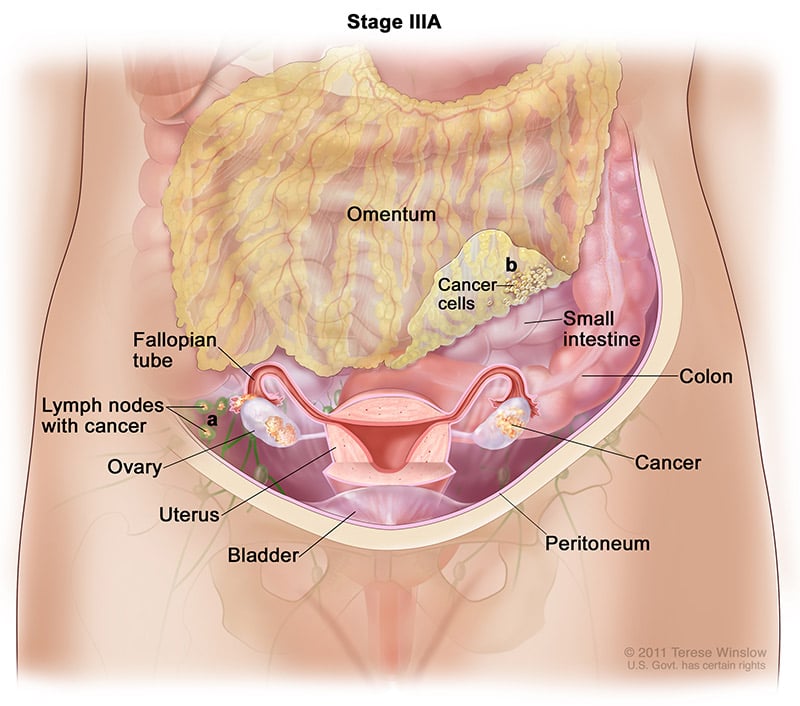
- Stage III: Cancer cells have spread to tissues outside the pelvis or to the regional lymph nodes. Cancer cells may be found on the outside of the liver.
-
Stage IIIA1: The cancer has spread to the retroperitoneal lymph nodes, which are found at the back of the abdomen, but not to the peritoneal surfaces.
-
Stage IIIA1(i): Metastases are 10 millimeters (mm) or smaller.
-
Stage IIIA1(ii): Metastases are larger than 10 mm.
-
-
Stage IIIA2: The cancer has spread microscopically from the pelvis to the abdomen. Cancer may or may not have spread to lymph nodes in the back of the abdomen.
-
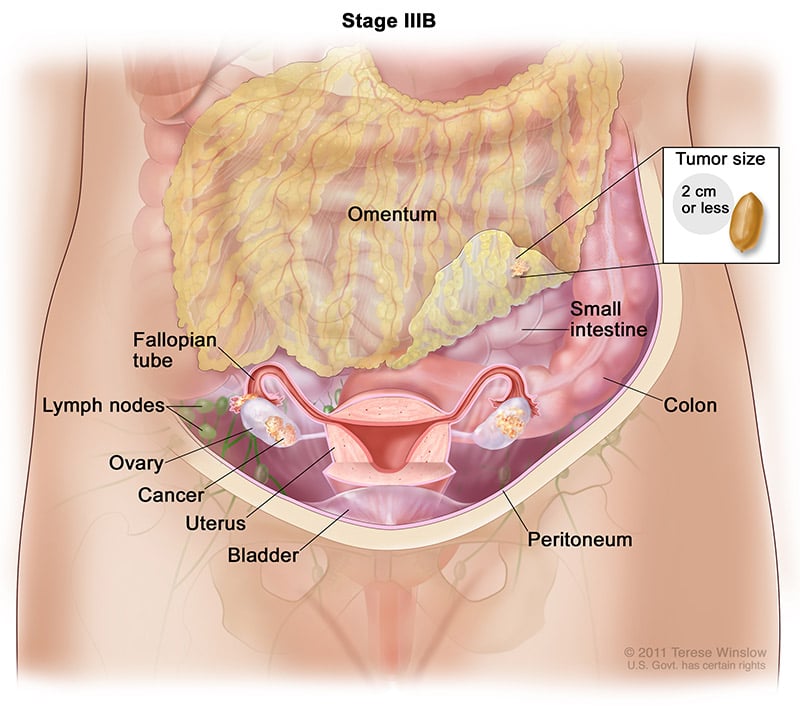
Stage IIIB: The cancer has visibly spread past the pelvis to the abdomen and is 2 centimeters (cm) or smaller, with or without spread to the retroperitoneal lymph nodes. A centimeter is roughly equal to the width of a standard pen or pencil.
-
Stage IIIC: The cancer has visibly spread past the pelvis to the abdomen and is larger than 2 cm, with or without spread to the retroperitoneal lymph nodes.

-
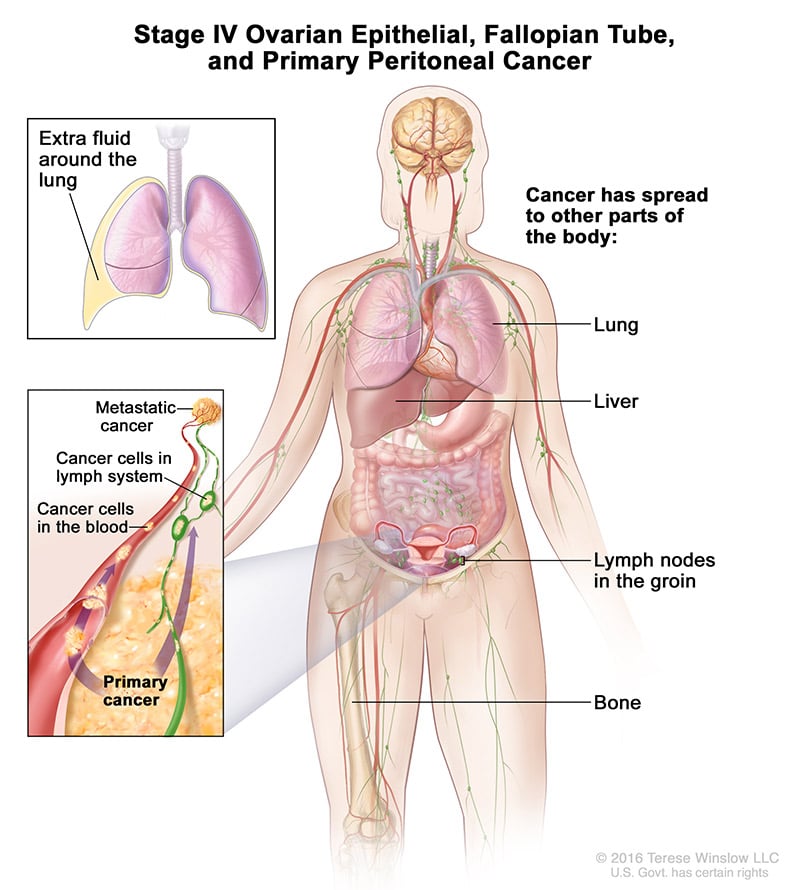
- Stage IV: Cancer cells have spread to tissues outside the abdomen and pelvis. Cancer cells may be found inside the liver, in the lungs, or in other organs.
-
Stage IVA: The cancer has spread to fluid around the lungs.
-
Stage IVB: The cancer has spread to the liver or spleen or to organs beyond the abdomen, including lymph nodes in the groin outside of the abdominal cavity.
-
Treatment Options
Your doctor can describe your treatment choices and the expected results. Most women have surgery and chemotherapy. Rarely, radiation therapy is used.
Cancer treatment can affect cancer cells in the pelvis, in the abdomen, or throughout the body:
- Local therapy: Surgery and radiation therapy are local therapies. They remove or destroy ovarian cancer in the pelvis. When ovarian cancer has spread to other parts of the body, local therapy may be used to control the disease in those specific areas.
- Intraperitoneal chemotherapy: Chemotherapy can be given directly into the abdomen and pelvis through a thin tube. The drugs destroy or control cancer in the abdomen and pelvis.
- Systemic chemotherapy: When chemotherapy is taken by mouth or injected into a vein, the drugs enter the bloodstream and destroy or control cancer throughout the body.
You may want to know how treatment may change your normal activities. You and your doctor can work together to develop a treatment plan that meets your medical and personal needs.
Surgery
The surgeon makes a long cut in the wall of the abdomen. This type of surgery is called a laparotomy. If ovarian cancer is found, the surgeon removes:
- both ovaries and fallopian tubes (salpingo-oophorectomy)
- the uterus (hysterectomy)
- the omentum (the thin, fatty pad of tissue that covers the intestines)
- nearby lymph nodes
- samples of tissue from the pelvis and abdomen
If the cancer has spread, the surgeon removes as much cancer as possible. This is called “debulking” surgery.
If you have early Stage I ovarian cancer, the extent of surgery may depend on whether you want to get pregnant and have children. Some women with very early ovarian cancer may decide with their doctor to have only one ovary, one fallopian tube, and the omentum removed.
Chemotherapy
Chemotherapy uses anticancer drugs to kill cancer cells. Most women have chemotherapy for ovarian cancer after surgery. Some women have chemotherapy before surgery.
Usually, more than one drug is given. Drugs for ovarian cancer can be given in different ways:
- By vein (IV): The drugs can be given through a thin tube inserted into a vein.
- By vein and directly into the abdomen: Some women get IV chemotherapy along with intraperitoneal (IP) chemotherapy. For IP chemotherapy, the drugs are given through a thin tube inserted into the abdomen.
- By mouth: Some drugs for ovarian cancer can be given by mouth.
Chemotherapy is given in cycles. Each treatment period is followed by a rest period. The length of the rest period and the number of cycles depend on the anticancer drugs used.
You may have your treatment in a clinic, at the doctor’s office, or at home. Some women may need to stay in the hospital during treatment.
Radiation Therapy
Radiation therapy is rarely used in the initial treatment of ovarian cancer, but it may be used to relieve pain and other problems caused by the disease. The treatment is given at a hospital or clinic. Each treatment takes only a few minutes.
Genetic Counseling To Determine High-Risk Inheritance
Genetic counseling is an important piece of our gynecological oncology program. Ovarian cancers, in particular, are sometimes associated with inheritable gene changes that increase the risk for types of cancer. Most well known is the association between ovarian cancer and mutations in genes BRCA1 and BRCA2, which also increases the risk for breast and prostate cancer. Finding a mutation in one of these genes may not only explain your current cancer but may guide your treatment, and allow us to tailor screening or preventative recommendations for you and for your family members. We recognize that discussing an increased risk for cancer for yourself and your family can be a difficult and intimidating process. Our genetic counselors will help you navigate the testing process and utilize the results to guide your care.
The Importance Of Connection
Our physicians collaborate with our nationally recognized supportive care services team to ensure that you and your family are connected to appropriate community resources, support groups and education classes. These licensed oncology clinical social workers are encouraging communicators and educators who provide a safe, supportive and open environment for patients to share feelings, learn coping strategies and explore ways to live as fully and joyfully as possible.
Colorado Ovarian Cancer Alliance
Among its many programs, Colorado Ovarian Cancer Alliance (COCA) provides newly diagnosed women with complimentary comfort kits of educational and support items, free, professionally-led support groups throughout the Denver and Boulder metro area and by phone, and one of the few financial assistance programs nationwide specifically for women in treatment for ovarian cancer. Rocky Mountain Cancer Centers has been a proud supporter of COCA and Jodi’s Race for Awareness for several years.
To find out more about all types of ovarian cancer, please visit the National Cancer Institute website or ask your cancer care team about your individual situation.